

Neurogenic Thoracic Outlet Syndrome: The Most Common Presentation
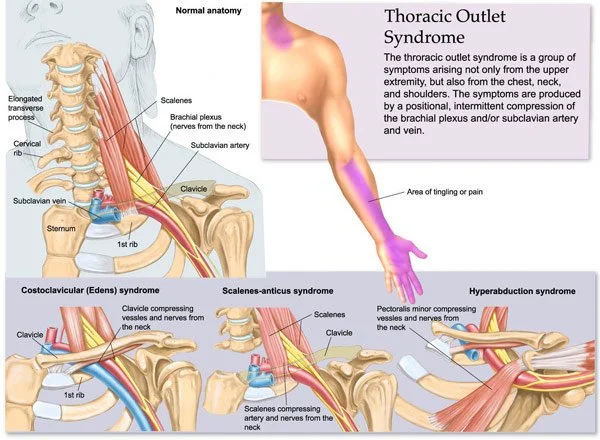
Neurogenic Thoracic Outlet Syndrome (nTOS) is the most frequently seen form of TOS, accounting for the vast majority of clinical cases. It involves compression or irritation of the brachial plexus, the network of nerves that supplies motor and sensory function to the upper limb.
Because nerves are highly sensitive to both mechanical pressure and tension, even subtle restrictions in the neck, chest, or shoulder can produce significant neurological symptoms.
Nerve Pain, Tingling, and Sensory Changes
The hallmark of neurogenic TOS is altered nerve sensation, often described by clients as tingling, numbness, burning, or “pins and needles” in the arm or hand. These symptoms are typically intermittent and strongly influenced by posture and activity.
A common clinical pattern involves symptoms radiating into the ulnar nerve distribution, affecting:
Ring finger
Little finger
Medial forearm
This occurs because the lower trunk of the brachial plexus (C8–T1 nerve fibers) is most commonly affected in thoracic outlet compression patterns.
Clients may also report:
Heaviness or fatigue in the arm
Weak grip strength or dropping objects
Increased symptoms with overhead activity or prolonged positioning
Relief when the arm is supported or posture is changed
Unlike vascular TOS, color changes or significant temperature differences are typically absent, though symptom intensity can still fluctuate significantly.
Why Nerves Become Irritated in TOS
Neurogenic symptoms are rarely caused by a single point of compression. Instead, they usually result from a combination of mechanical narrowing and increased neural tension along the nerve pathway.
Key contributing factors include:
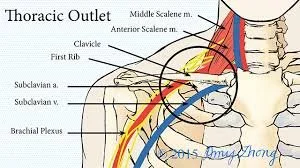
Tight anterior and middle scalenes increasing interscalene space tension
Shortened pectoralis minor altering scapular position and reducing subclavicular space
Fascial restriction through the anterior neck and chest
Postural patterns such as forward head posture and rounded shoulders
Repetitive overhead or sustained arm positioning
These factors can reduce available space for the brachial plexus and increase sensitivity of the nerve tissue, leading to symptoms that may vary day to day.
Clinical Massage Therapy Perspective
From a clinical massage therapy standpoint, neurogenic TOS is particularly relevant because much of the dysfunction involves soft tissue restriction influencing nerve mechanics.
Treatment is typically directed at reducing tension in key muscular structures, including:
Scalenes (reducing interscalene compression influence)
Pectoralis minor (improving scapular positioning and anterior shoulder space)
Subscapularis (addressing anterior shoulder tightness and internal rotation bias)
By addressing these areas, manual therapy may help improve:
Tissue mobility around nerve pathways
Overall shoulder girdle alignment
Comfort with movement and posture
Reduction in nerve irritation symptoms such as tingling or heaviness
While massage therapy does not directly “treat” the nerve itself, it plays a valuable role in reducing the mechanical and soft tissue factors that contribute to nerve sensitivity.
Key Clinical Insight
Neurogenic TOS is often a multifactorial and movement-dependent condition, meaning symptoms are not constant but change with posture, activity, and muscular load. This variability is one of the reasons it can be difficult to diagnose and why a thorough clinical assessment is essential.
Understanding the relationship between nerve pathways and surrounding soft tissue structures is critical in both assessment and treatment planning.